
Translate this page into:
Prevalence of Anemia in Saudi Women of Reproductive Age and its Association with a Family History of Anemia in Makkah, Saudi Arabia
 PhD., Arwa Y. Zakri2MSc, Amir Elmubarek Ali1Ph.D., Samah Labban1Ph.D., Dareen Mattar1Ph.D., Aisha Azmat1MPHil MSc, Wahaj. A. Khan3Ph.D, Mohamed Osman Elamin3,Ph.D, Ahmed A. Osman4MD
PhD., Arwa Y. Zakri2MSc, Amir Elmubarek Ali1Ph.D., Samah Labban1Ph.D., Dareen Mattar1Ph.D., Aisha Azmat1MPHil MSc, Wahaj. A. Khan3Ph.D, Mohamed Osman Elamin3,Ph.D, Ahmed A. Osman4MD

*Corresponding author: Mohamed Osman Elamin, Department of Environmental and Occupational Health, Faculty of Public Health and Informatics, Umm Al-Qura University, Makkah, Saudi Arabia. me1832092@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Albar HT, Zakri A, Elmubarek Ali A, Labban S, Mattar D, Azmat A, et al. Prevalence of Anemia in Saudi Women of Reproductive Age and its Association with a Family History of Anemia in Makkah, Saudi Arabia. Glob J Med Pharm Biomed Update. 2025;20:7. doi: 10.25259/GJMPBU_3_2025
Abstract
Objectives:
Anemia is a widespread public health issue, especially among women of reproductive age, influenced by physiological, nutritional, and socioeconomic factors. Familial history and genetic predisposition may play critical roles in its prevalence. This study investigates the impact of familial history and sociodemographic factors on anemia among Saudi women, emphasizing preventive strategies for high-risk groups.
Material and Methods:
A cross-sectional study was conducted with 809 women aged 12–49 years residing in Makkah, Saudi Arabia. An electronic questionnaire was used to collect data on anemia prevalence, familial history, and sociodemographic variables. Statistical analyses were employed to determine associations between anemia and these factors.
Results:
The prevalence of anemia was 57% (461 respondents). A statistically significant association was found between familial history and anemia prevalence (P < 0.001). However, no significant correlations were identified between anemia and educational attainment, marital status, income, medication use, or chronic illnesses.
Conclusion:
Familial history significantly influences anemia prevalence among Saudi women, emphasizing the need for early detection and management in genetically predisposed individuals. Public health interventions should focus on raising awareness, implementing screening programs, and adopting preventive strategies for high-risk populations.
Keywords
Anemia
Family history
Reproductive age
Women

INTRODUCTION
Anemia is defined as a reduced hemoglobin level (Hb) – below 13 g/dL for men and 12 g/dL for women – or a low hematocrit or red blood cell (RBC) count.[1] It occurs when there is an inadequate number of red blood corpuscles to meet physiological needs.[2] Anemia is a very common health problem that may affect people at any age in both developing and developed countries. Anemia is often associated with iron deficiency, the most common cause worldwide. Pregnant women, women of reproductive age (WRA), and children are at an increased risk of developing anemia.[2,3] WRA are physiologically more susceptible to anemia due to chronic heavy menstrual blood loss (menorrhagia), repeated childbearing, and pregnancy demands.[3] In 2016, the World Health Organization (WHO) estimated that anemia affected about 33% of WRA globally.[4] Anemia impairs the capacity of the blood to transport oxygen to tissues.[5] Complications of anemia range from mild to severe and can include headaches, fatigue, low productivity, and maternal mortality. In 2002, the WHO reported that anemia was considered one of the top 10 mortality risks.[6,7] Anemia has three main mechanisms: (1) Excessive blood loss (e.g., acute bleeding or chronic low-volume loss), (2) extreme RBC destruction (hemolysis), and (3) deficient production of RBCs (ineffective hematopoiesis).[8] The most common cause of anemia is poor nutrition, mostly due to a deficiency in iron, folic acid, or vitamin B12. Other causes of anemia include inherited anemia (e.g., sickle cell and thalassemia) or autoimmune (hemolytic anemia). Anemia can also be associated with family history, infection (malaria), demographic-related factors (age and gender), malabsorption (achlorhydria), environmental pollutants (lead exposure), socioeconomic factors (low maternal level of education or low household income), and chronic diseases (cancer).[9] Moreover, anemia is often associated with chronic diseases, including hypothyroidism, hypertension, rheumatism, and heart failure.[10,11]
Anemia occurs in people of any age; however, women of childbearing age and young children are especially susceptible.[9] Anemia is associated with poor immunity, cognitive dysfunction, decreased ability to work, and reduced overall quality of life.[12,13] During childhood, all bone marrow is hematopoietic, whereas hematopoietic marrow is restricted to the axial skeleton in adults. Therefore, Hb concentrations are higher in children than in adults.[14] The WHO estimates that 24.8% of the world’s population suffers from anemia, which amounts to about 1.62 billion people.[15] It has been reported that the highest prevalence of anemia was found in preschoolage children (47.4%), while the prevalence of anemia in men (12.7%) was the lowest.[16] Approximately 32.4 million pregnant women around the world suffer from anemia. For all WRA, the prevalence of anemia is about 29% (528.7 million WRA).[16] The WHO has reported that anemia was observed in 40% of Saudi WRA. Another study found that 32.3% of non-pregnant women of childbearing age in Saudi Arabia suffered from anemia.[15,17] The female reproductive years are between menarche (the first menstrual cycle) and menopause (the cessation of menses for 12 consecutive months). According to the American community, the years between menarche and menopause fall roughly between age 12 and age 49.[18] Previously, it was revealed that having a family history of iron deficiency anemia was associated with an increased risk of anemia.[19] However, little data are available about the prevalence of anemia in women with a family history of anemia in the Saudi population.
Most research concerning anemia in Saudi Arabia has focused on preschool children under six and their nutritional status.[20,21] Some hospital-based studies on the prevalence and risk factors for anemia have been conducted in Saudi Arabia;[20-23] however, these studies are subjected to selection bias and cannot be generalized. Therefore, the present study aimed to estimate the prevalence of anemia in women with a family history of anemia in Makkah.
Highlight of study
The study highlights anemia’s 57% prevalence among Saudi WRA, with familial history being a significant risk factor. Preventive strategies targeting genetically predisposed groups are emphasized, alongside the need for public health interventions, awareness programs, and early screening to mitigate anemia’s impact.
MATERIAL AND METHODS
Study design
This cross-sectional study was conducted in Makkah, Saudi Arabia, between March and June 2022. The research aimed to examine the prevalence and associated factors of anemia among Saudi women aged 12–49 years with a family history of the condition. Utilizing an electronic questionnaire, data were collected from 809 participants during this period. The study’s timeframe allowed for a comprehensive analysis, providing valuable insights into the burden of anemia and its relationship with familial and sociodemographic factors.
Study population
The study targeted WRA, defined as those between 12 and 49 years, residing in Makkah, Saudi Arabia. Eligibility criteria included residency in Makkah, consent to participate, and willingness to complete the electronic questionnaire. Anemia among WRA was classified based on Hb concentrations below 12.0 g/dL, in accordance with established diagnostic criteria.[24] This threshold aligns with global standards for identifying anemia in non-pregnant women, enabling consistent evaluation of its prevalence. The inclusion criteria ensured a focused and representative sample, while the standardized definition of anemia facilitated comparability with existing research on women’s health in similar contexts.
Sample size and sampling
The sample size of this research was determined using the Steven K. Thompson formula:[25]
Where: Where NNN represents the population size, ppp denotes the probability value (0.5), ddd indicates the margin of error (0.05), and ZZZ corresponds to the standard normal value (1.96). Applying this formula, a total sample size of 809 Saudi WRA (12–49 years) residing in Makkah, Saudi Arabia, was determined, ensuring sufficient statistical power for the analysis.
Data collection tools, procedures, and data quality management
Interview questionnaire
Data collection was conducted through an Arabic-language electronic questionnaire distributed through social media platforms to reach the study population. The structured and validated questionnaire consisted of 29 items divided into three sections: A consent form, sociodemographic information, and a family history of anemia, as well as questions addressing anemia status, chronic diseases, medication use, and vitamin intake. The questionnaire was adapted from a prior study conducted in Thatta, Pakistan.[23] To ensure clarity and relevance, a pilot study was performed involving 30 Saudi WRA (12–49 years) residing in Makkah; these participants were excluded from the final analysis and sample size. Reliability testing using Cronbach’s Alpha yielded a score of 0.72, reflecting good internal consistency. Anemia severity was categorized based on Hb levels: [26] Mild (10.0 g/dL to the lower limit of normal), moderate (8.0–10.0 g/dL), severe (6.5–7.9 g/dL), and life-threatening (<6.5 g/dL). This classification provided a framework for evaluating the condition’s impact and identifying critical cases. The methodological rigor of the study ensures the reliability and validity of the collected data, facilitating a robust analysis of anemia prevalence and its associated factors among Saudi women in the target population.
Anthropometric data collection
Each participant was instructed to measure their weight and height while barefoot and dressed in minimal outerwear, ensuring consistency in data collection. These measurements were recorded directly into the questionnaire. Subsequently, the mass index (BMI) for each individual was calculated using the standard formula: Body mass (kg) divided by height squared (m2). The computed BMI values were then categorized in accordance with the WHO classification criteria for overweight and obesity. This approach aligns with established global standards, ensuring the reliability and comparability of the anthropometric data. By adhering to the WHO guidelines, the study aims to provide robust insights into weight-related health risks while minimizing potential measurement biases. The reliance on self-reported data was mitigated by clear instructions, allowing participants to accurately document their anthropometric details and ensuring that the BMI classifications reflect an objective and systematic methodology.
Statistical methods
The data were collected, coded, and entered into the statistical software program Statistical Package for the Social Sciences version 19 (IBM, Chicago, IL, USA). All statistical analyses were conducted using the Chi-square test. A P ≤ 0.05 was considered statistically significant. Descriptive analysis based on frequency and percent distribution was performed for all categorical variables, while means with standard deviations and medians were used to display numerical variables.
RESULTS
Sociodemographic characteristics
A total of 809 eligible participants completed and submitted the questionnaire. The data presented here showed the frequency distribution and percentage of sociodemographic and lifestyle characteristics of the study subjects (n = 809). We observed that the majority of the participants (35.5%) were between the ages of 22 and 31 years, followed by those aged <20 years (12.2%) and those aged >30 years (32.6%), while 19.7% participants were aged between 42 and 49 years. Our study found that the younger demographic, specifically those between the ages of 22 and 31 years, made up the largest portion of participants. Interestingly, the age group of <20 years also had a significant representation in our study, indicating a diverse range of ages among our participants. In addition, the data showed a fairly even distribution among participants aged >30 years and those aged between 42 and 49 years.
Moreover, the majority of the participants had a bachelor’s degree (68.23%), whereas 0.12% of the participants had a diploma, and 14.8% of the participants held a secondary school certificate. In addition, 12.86% were postgraduate students, 3.46% were intermediate students, and 0.49% were in elementary schools. We found that a considerable number of participants were working (42.0%), non-working (39.2%), and students (17.9%). It is important to consider that having a higher education level does not necessarily correlate with being employed, as factors such as job market conditions and personal circumstances play a significant role in employment status.[27] Being a student does not preclude someone from being employed, as many individuals’ balance work and education simultaneously. The majority of the participants reported a monthly income of <5,000 Saudi Riyal (52.41%), while 21.38% of the participants had a monthly income ranging between 5,000 and 10,000 SR, and (26.21%) had a monthly income higher than 10,000 SR. The percentage of married, widowed, single, and divorced participants was (32%), (60%), (6.3%), and (1.4%), respectively. The results indicated that among the participants, 92.21% identified as non-smokers, a factor potentially protective against anemia, as smoking can contribute to chronic inflammation and iron metabolism disruption.[28] In addition, 40.79% reported having undergone prior surgeries, ranging from appendectomy to hysterectomy. Surgical histories, particularly procedures involving significant blood loss or affecting the gastrointestinal system (e.g., sleeve gastrectomy or cholecystectomy), may contribute to the development or exacerbation of anemia. For instance, surgeries like sleeve gastrectomy can lead to nutrient malabsorption, including iron and vitamin B12, critical components in Hb synthesis.[29] Similarly, conditions necessitating surgeries like fibrous tumor removal or hysterectomy often involve heavy menstrual bleeding, a well-known risk factor for anemia.[30] This distribution underscores the importance of pre-operative and post-operative screening for anemia, especially among women, to facilitate early intervention and prevent complications arising from undiagnosed or unmanaged anemic conditions [Table 1].
| Characteristics | Variables | Subjects | |
|---|---|---|---|
| Frequency | (%) | ||
| Age group | 12–21 | 99 | 12.2 |
| 22–31 | 287 | 35.5 | |
| 32–41 | 264 | 32.6 | |
| 42–49 | 159 | 19.7 | |
| Education level | Bachelor | 552 | 68.23 |
| Diploma | 1 | 0.12 | |
| Secondary School | 120 | 14. 83 | |
| Postgraduate | 104 | 12.86 | |
| Intermediate | 28 | 3.46 | |
| Elementary | 4 | 0.49 | |
| Work status | Unemployed | 317 | 39.2 |
| Employed | 340 | 42.0 | |
| Student | 145 | 17.9 | |
| Other | 7 | 0.9 | |
| Monthly Income | More than 10,000 SR | 212 | 26.21 |
| 5,000–10,000 SR | 173 | 21.38 | |
| <5,000 SR | 424 | 52.41 | |
| Marital Status | Single | 264 | 32.6 |
| Married | 483 | 59.7 | |
| Divorced | 51 | 6.3 | |
| Widowed | 11 | 1.4 | |
| BMI | Underweight <18.5 | 64 | 7.9 |
| Normal range 18.5–24.9 | 348 | 43.3 | |
| Overweight 25.0–29.9 | 236 | 29.3 | |
| Obese ≥30 | 156 | 19.4 | |
| Smoking Status | Smoker | 63 | 7.79 |
| Non-smoker | 746 | 92.21 | |
| Surgery Status * | Had a prior surgery | 330 | 40.79 |
| No prior surgery | 479 | 59.21 | |
Pregnancy-related characteristics
Approximately 75% of the participants had fewer than four children, while 25% had more than four children. One participant had nine children. Moreover, the data showed that 38% of the married participants had a history of miscarriage and that puberty ranged from 9 to 15 years (93%) and the participants reported starting puberty between the ages of 10 and 14. The study also found that 62% of the participants had pursued higher education after completing high school. Overall, the data provide a comprehensive picture of the demographics and experiences of the participants in the study [Table 2].
| Characteristics | Variables | Subjects | |
|---|---|---|---|
| Frequency | (%) | ||
| Puberty age | 8–11 | 105 | 12.9 |
| 12–15 | 653 | 80.71 | |
| 16–19 | 49 | 6 | |
| 20–23 | 2 | 0.25 | |
| Number of miscarriages | No miscarriages | 609 | 75.5 |
| 1 | 118 | 14.6 | |
| 2 | 54 | 6.7 | |
| 3 | 19 | 2.35 | |
| 4 | 6 | 0.74 | |
| 7 | 1 | 0.12 | |
| Number of children | 0 | 401 | 49.69 |
| 1 | 78 | 9.67 | |
| 2 | 95 | 11.77 | |
| 3 | 99 | 12.26 | |
| 4 | 73 | 9.04 | |
| 5 | 74 | 9.17 | |
| 6 | 29 | 3.59 | |
| 7 | 7 | 0.87 | |
| 8 | 4 | 0.49 | |
| 9 | 1 | 0.12 | |
Prevalence of anemia
The prevalence of anemia (low Hb level) and its severity are shown in Figure 1. The data show that 291 (63%) participants had mild anemia (10–12 g/dL), 141 (30%) had moderate anemia (8–10 g/dL), 15 (3%) had severe anemia (6.5–7.9 g/dL), and 14 (3%) had life-threatening (<6.5 g/dL) anemia. The prevalence of anemia in the entire sample was (57%). These findings highlight the significant burden of anemia in this population, with most participants experiencing mild to moderate levels of the condition. The data also imply the importance of addressing anemia as a public health concern, particularly in populations at risk for nutritional deficiencies or other health conditions that can contribute to low Hb levels [Figure 1].
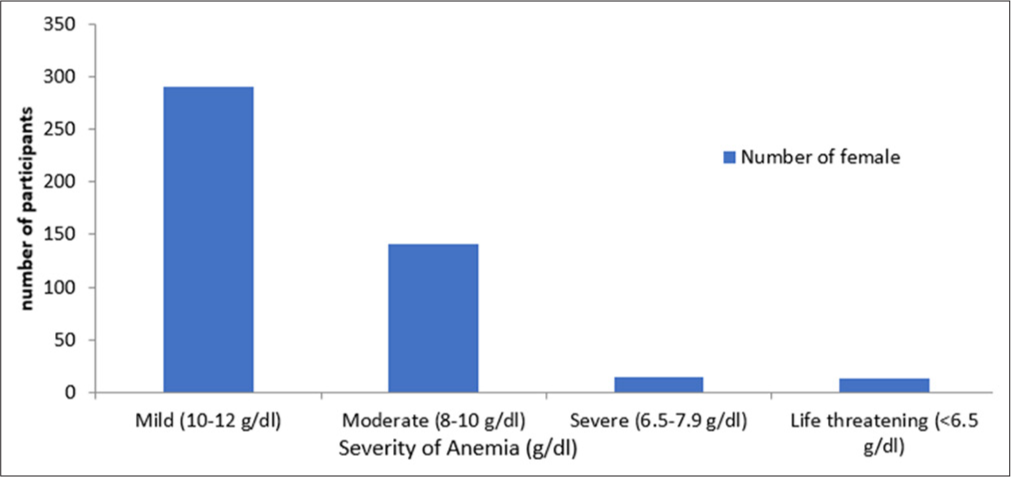
- The prevalence of anemia (low hemoglobin level) and its severity in participants (n = 807).
The association of anemia with various factors and family history
Further analysis was conducted using the Chi-square test to examine the association between anemia prevalence among participants and various socioeconomic factors. The results revealed no statistically significant relationship between anemia and the investigated socioeconomic variables, as indicated by a P > 0.05. Similarly, the associations between anemia, chronic disease (hypothyroidism, hypertension, rheumatism, diabetes mellitus, and chronic respiratory diseases), and medication use were found to be statistically non-significant (P > 0.05). However, a statistically significant relationship emerged between anemia and a familial history of the condition (P < 0.000). To further explore this association, the Pearson correlation coefficient test was employed, which demonstrated a strong and statistically significant correlation between anemia and a family history of hereditary blood disorders, specifically sickle cell anemia and thalassemia (P < 0.000). These findings, as presented in Table 3, underscore the pivotal role of genetic predisposition in the development of anemia. While socioeconomic factors and chronic disease did not exhibit a direct relationship, the clear linkage to familial history highlights the importance of genetic screening and early intervention strategies. These results provide a compelling case for prioritizing family history in the assessment and management of anemia, especially in regions where hereditary blood disorders are prevalent.
| Factor | Pearson’s Chi-squared test | Significance level |
|---|---|---|
| Age | 1.755 | 0.882 |
| Marital status | 3.880 | 0.275 |
| Income | 1.191 | 0.551 |
| Chronic disease | 0.029 | 0.413 |
| Medication use | 0.092 | 0.761 |
| Family history factor | 0.299 | 0.000* |
| History factors (sickle cell anemia and thalassemia) | 0.151 | 0.000* |
The Pearson correlation coefficient test was used to check the relation between anemia and family history factors and there was an excellent positive, statistically significant correlation between anemia and family history factor since (significance = 0.000), which is less than the significant level (a = 0.05) as shown in [Table 4].
| Anemia | |
|---|---|
| Family history factor | |
| Pearson Correlation | 0.299** |
| Sig. (two-tailed) | 0.000 |
| Number | 809 |
DISCUSSION
This is one of the first studies conducted in Makkah, KSA to measure the burden of anemia among women with a family history of anemia. Our study specifically focuses on WRA (12–49 years) because this population is at a significantly higher risk of anemia due to menstrual blood loss, pregnancy, and increased iron demands. The WHO recognizes anemia as a major public health concern among reproductiveage women, particularly in regions with high rates of iron deficiency and nutritional anemia.[31] Several studies have documented that anemia prevalence is notably high among adolescents and young women, particularly in Middle Eastern populations, including Saudi Arabia.[32,33] Factors such as dietary habits, menstrual blood loss, pregnancy, and family history play a crucial role in this group, making it a relevant and necessary focus of investigation. While anemia does increase with age, our study’s primary aim is to assess its prevalence in reproductive-age women and its association with family history. The findings provide critical insights into preventative and interventional strategies targeting this vulnerable age group, ultimately helping to reduce anemia-related complications in later life.
Global data (WHO) indicate that anemia is notably prevalent among younger populations, particularly children under five and WRA (15–49 years). According to the WHO, in 2019, 39.8% of children aged 6–59 months and 29.9% of women aged 15–49 years were affected by anemia.[34] A comprehensive study analyzing data from 47 low- and middle-income countries between 2010 and 2018 found that 64.3% of children aged 6–35 months and 46.8% of those aged 36–59 months were anemic, highlighting a higher prevalence in younger children.[35] Furthermore, a 2023 study published in The Lancet Haematology reported that in 2021, 46% of women globally were anemic, with the prevalence rising to 33.7% among women aged 15– 49 years.[36] These statistics underscore that anemia is particularly prevalent among younger age groups, especially children under five and WRA, emphasizing the importance of focusing on these populations in anemia-related research and interventions. Another study reported that 49.5% of women aged 15–49 years were anemic, with factors such as education level, socioeconomic status, and dietary habits significantly influencing anemia prevalence.[37] A study found that 54.3% of non-pregnant, non-lactating women aged 18–49 were anemic. Iron deficiency was prevalent in 86.9% of participants, underscoring the need for targeted interventions.[38] A research study identified a 59.06% prevalence of anemia among women aged 15–49, with higher rates observed in pregnant women. Factors such as educational status, menstrual irregularities, and low body weight were significantly associated with anemia.[39] Thus, anemia remains a significant public health concern among WRA (12–49 years), with global studies consistently reporting high prevalence rates in this population. The evidence highlights that nutritional deficiencies, menstrual blood loss, pregnancy, and socioeconomic factors are key contributors to anemia in younger women, often exceeding the rates seen in older populations. Addressing anemia in this age group is crucial for improving maternal and child health outcomes, reducing long-term complications, and preventing its persistence into older adulthood. The study found that anemia remains a public health issue, with a high prevalence of anemia (57%) of participants who were residing in Makkah. These results are consistent with those of previous studies that showed the prevalence of iron-deficiency anemia among female Saudi university students.[15,17,40] Further research is needed to explore the underlying causes of anemia in this population as well as to develop targeted interventions to address this issue. Education and awareness campaigns may be necessary to increase knowledge about anemia and promote healthy lifestyle choices that can help prevent and manage the condition. Collaboration between healthcare providers, policymakers, and community leaders will be essential in addressing the burden of anemia among women in Makkah and improving overall health outcomes in the region.
The results of the current study showed statistically significant association between anemia and socioeconomic or educational factors, including marital status and income. These results are consistent with those of a previous study that found that demographic or socioeconomic factors[41,42] and anthropometric status were not associated with any type of anemia.[43] Efforts should be made to increase awareness about anemia and its potential impact on overall health. By working together, healthcare providers, policymakers, and community leaders can create a comprehensive approach to addressing anemia and improving the well-being of women in the region. The results of the current study showed a positive, statistically significant correlation between anemia and family history factors at the statistical level (a = 0.05). Previously, it was reported that genetic Hb disorders (e.g., sickle cell anemia and thalassemia) in family members played a role in the occurrence of anemia.[44] Several previous Saudi Arabian studies reported that a family history of anemia created a significantly heightened risk of anemia in individuals. Another study suggested that a family history of anemia (iron deficiency) was significantly associated with an increased risk of anemia in adolescents, which might be similar to the other disorders.[45]
A limitation of this study was that we could not compare the results of this study with similar studies conducted in other regions of Saudi Arabia, as few studies have focused on this topic. Data gathered through self-recall questionnaires may be subject to various biases that may affect the validity and reliability of the data collected. Future studies should aim to obtain objective levels of hemoglobin (HGB). Clearly, future approaches to prevent and control anemia should include detailed epidemiological studies to determine the causes of anemia in this population.
CONCLUSION
In the current study, 57% of our sample of Saudi WRA in Makkah had anemia. The findings indicated a statistically significant correlation between anemia and family history factors. However, no significant correlation was found between the presence of anemia and socioeconomic factors, such as marital status and income, or with chronic disease or medication use. Clearly, future approaches to prevent and control anemia should target the population with a family history of anemia. We recommend conducting more studies in Makkah with a large sample and conducting more studies in different regions of the Kingdom of Saudi Arabia and comparing the results with those of our research on anemia in the Makkah region.
Author’s contributions:
All the authors contributed equally.
Ethical approval:
Ethical approval for this study was obtained from the Institutional Research Board (IRB) at Umm Al-Qura University, number HAPO-02-K-012-2022-03-990, dated 3rd March 2022.
Declaration of patient consent:
Patient’s consent is not required as there are no patients in this study.
Conflicts of interest:
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation:
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity Geneva: World Health Organization; 2011.
- [Google Scholar]
- Determining Factors for the Prevalence of Anemia in Women of Reproductive Age in Nepal: Evidence from Recent National Survey Data. PLoS One. 2019;14:e0218288.
- [CrossRef] [PubMed] [Google Scholar]
- Iron Status and Reproduction in US Women: National Health and Nutrition Examination Survey, 1999-2006. PLoS One. 2014;9:e112216.
- [CrossRef] [PubMed] [Google Scholar]
- Tools for Effective Prevention and Control Geneva, Switzerland: World Health Organization; 2017. p. :1-83.
- [Google Scholar]
- Worldwide Prevalence of Anaemia, WHO Vitamin and Mineral Nutrition Information System, 1993-2005. Public Health Nutr. 2009;12:444-54.
- [CrossRef] [PubMed] [Google Scholar]
- A Systematic Analysis of Global Anemia Burden from 1990 to 2010. Blood. 2014;123:615-24.
- [CrossRef] [PubMed] [Google Scholar]
- Global Health Risks: Mortality and Burden of Disease Attributable to Selected Major Risks In: World Health Organization. 2009.
- [Google Scholar]
- Awareness of Anemia Causes among Saudi Population in Qassim Region, Saudi Arabia. Natl J Integr Res Med. 2013;4:35-40.
- [Google Scholar]
- The Pattern of Iron Deficiency with and without Anemia among Medical College Girl Students in High Altitude Southern Saudi Arabia. J Family Med Prim Care. 2020;9:5018-25.
- [CrossRef] [PubMed] [Google Scholar]
- Role of Iron Deficiency in Heart Failure-Clinical and Treatment Approach: An Overview. Diagnostics (Basel). 2023;13:304.
- [CrossRef] [PubMed] [Google Scholar]
- Iron Deficiency Anemia, Population Health and Frailty in a Modern Portuguese Skeletal Sample. PLoS One. 2019;14:e0213369.
- [CrossRef] [PubMed] [Google Scholar]
- Comprehensive Anaemia Programme and Personalized Therapies (CAPPT): Protocol for a cluster-Randomised Controlled Trial Testing the Effect Women's Groups, Home Counselling and Iron Supplementation on Haemoglobin in Pregnancy in Southern Nepal. Trials. 2022;23:183.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence and Risk Factors of Anaemia among Ever-married Women in Jordan. East Mediterr Health J. 2019;25:543-52.
- [CrossRef] [PubMed] [Google Scholar]
- Normal Appearances, Variants and Diffuse Disease States In: Pediatric and Adult MRI Atlas of Bone Marrow. 2016.
- [CrossRef] [Google Scholar]
- The Prevalence of Iron Deficiency Anemia in a Saudi University Female Students. J Microsc Ultrastruct. 2015;3:25-8.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of Anemia and Correlated Factors in the Reproductive Age Women in Rural Areas of Tabas. J Family Reprod Health. 2013;7:139-44.
- [Google Scholar]
- Anemia and Iron Intake of Adult Saudis in Riyadh City, Saudi Arabia. Pak J Nutr. 2007;6:355-8.
- [CrossRef] [Google Scholar]
- Physiology, Female Reproduction In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2025.
- [Google Scholar]
- Prevalence of Anemia And Associated Factors In Childbearing Age Women in Riyadh, Saudi Arabia. J Nutr Metab. 2013;2013:636585.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of Anemia among Saudi Patients with Solid Cancers at Diagnosis in King Faisal Hospital, Taif Province, Kingdom of Saudi Arabia. PLoS One. 2021;16:e0246202.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of Iron Deficiency Anemia among Female Elementary School Children in Northern Jeddah, Saudi Arabia. Med Sci. 2008;15:32-7.
- [CrossRef] [Google Scholar]
- Evaluation of Prevalence and Pattern of Anemia-A hospital-based Study in Aseer Province, Kingdom of Saudi Arabia. J Exp Med Surg Res. 2013;2:32-5.
- [Google Scholar]
- Prevalence and Determinants of Anemia among Women of Reproductive Age in Thatta Pakistan: Findings from a Cross-Sectional Study. PLoS One. 2020;15:e0239320.
- [CrossRef] [PubMed] [Google Scholar]
- Knowledge about the Prevalence of Iron Deficiency Anemia and Its Associated Risk Factors in Females in Saudi Arabia. Egypt J Hosp Med. 2018;73:6983-6.
- [CrossRef] [Google Scholar]
- Sample size for estimating multinomial proportions. Am Stat. 1987;41:42-6.
- [CrossRef] [Google Scholar]
- Chronic Anemia (Nursing) In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2023.
- [Google Scholar]
- COVID-19 Employment Status, Dyadic Family Relationships, and Child Psychological Well-Being. J Adolesc Health. 2021;69:705-12.
- [CrossRef] [PubMed] [Google Scholar]
- Anemia of Inflammation and Iron Metabolism in Chronic Diseases. Rev Clin Esp (Barc). 2024;224:598-608.
- [CrossRef] [PubMed] [Google Scholar]
- Nutritional Implications in Preparing Patients for Total Gastrectomy. Curr Surg Rep. 2020;8:1-7.
- [CrossRef] [Google Scholar]
- Endometrial Resection and Ablation Versus Hysterectomy for Heavy Menstrual Bleeding. Cochrane Database Syst Rev. 2021;2:CD000329.
- [CrossRef] [PubMed] [Google Scholar]
- Overview of Iron Deficiency and Iron Deficiency Anemia in Women and Girls of Reproductive Age. Int J Gynaecol Obstet. 2023;162(Suppl 2):78-82.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence and Factors Associated with Dyslipidemia among Adolescents in Saudi Arabia. Sci Rep. 2022;12:16888.
- [CrossRef] [PubMed] [Google Scholar]
- Metabolic Syndrome: Prevalence and Risk Factors among Adolescent Female Intermediate and Secondary Students in Saudi Arabia. Int J Environ Res Public Health. 2021;18:2142.
- [CrossRef] [PubMed] [Google Scholar]
- National, Regional, and Global Estimates of Anaemia by Severity in Women and Children for 2000-19: A Pooled Analysis of Population-representative Data. Lancet Glob Health. 2022;10:e627-39.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence and Changes of Anemia among Young Children and Women in 47 Low-and Middle-income Countries, 2000-2018. EClinicalMedicine. 2021;41:101136.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence, Years Lived with Disability, and Trends in Anaemia Burden by Severity and Cause, 1990-2021: Findings from the Global Burden of Disease Study 2021. Lancet Haematol. 2023;10:e713-34.
- [Google Scholar]
- Anaemia Prevalence and Socio-demographic Factors among Women of Reproductive Age (WRA): A Geospatial Analysis of Empowered Action Group (EAG) States in India. Spat Spatiotemporal Epidemiol. 2024;49:100644.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of Anemia Among Women of Reproductive Age in Rural Haryana, India. Curr Dev Nutr. 2021;5(Suppl 2):699.
- [CrossRef] [Google Scholar]
- Anemia among Women of Reproductive Age: A Cross Sectional Study in Sub District Hospital, Akhnoor. Int J Reprod Contracept Obst Gynecol. 2021;10:2662-7.
- [CrossRef] [Google Scholar]
- Prevalence of Undiagnosed Iron Deficiency Anemia and Associated Factors among Female Undergraduate Medical Students in Makkah, Saudi Arabia. Cureus. 2023;15:e50046.
- [CrossRef] [PubMed] [Google Scholar]
- Anaemia in Low-Income and Middle-income Countries. Lancet. 2011;378:2123-35.
- [CrossRef] [PubMed] [Google Scholar]
- Anemia Association with Socio-Demographic and Dietary Related Factors among Women of Childbearing Age: A Review Article. J Health Rehabil Res. 2023;3:1078-84.
- [CrossRef] [Google Scholar]
- Anaemia and Its Relation to Demographic, Socio-economic and Anthropometric Factors in Rural Primary School Children in Hai Phong City, Vietnam. Nutrients. 2019;11:1478.
- [CrossRef] [PubMed] [Google Scholar]
- Knowledge and Attitude Toward Donot-Resuscitate among Patients and Their Relatives Visiting Outpatient Clinics at King Abdulaziz University Hospital, Jeddah, Saudi Arabia. Saudi Med J. 2020;41:53-8.
- [CrossRef] [PubMed] [Google Scholar]
- May-Thurner Syndrome: A Forgotten Cause of Venous Thromboembolism. Indian J Crit Care Med. 2020;24:66-8.
- [CrossRef] [PubMed] [Google Scholar]




