
Translate this page into:
Efficacy of Piroxicam and Tramadol for Relieving Pain Associated with Therapeutic Dental Extractions followed by Immediate Archwire Loading during Orthodontic Treatment: A Cross-Over Randomized Clinical Trial
 BDS, Madhu Sweta Jain1BDS, Hitesh Ramdas Sawant1MDS, Parag Vishnu Gangurde1MDS, Viraj Rajeev Kharkar2MDS, Harjit Singh Kalsi2MDS, Sanpreet Singh Sachdev3,MDS
BDS, Madhu Sweta Jain1BDS, Hitesh Ramdas Sawant1MDS, Parag Vishnu Gangurde1MDS, Viraj Rajeev Kharkar2MDS, Harjit Singh Kalsi2MDS, Sanpreet Singh Sachdev3,MDS

*Corresponding author: Sanpreet Singh Sachdev, Department of Oral Pathology and Microbiology, Bharati Vidyapeeth (Deemed to be University) Dental College and Hospital, Navi Mumbai, Maharashtra, India. sunpreetss@yahoo.in
-
Received: ,
Accepted: ,
How to cite this article: Tiwari A, Jain MS, Sawant HR, Gangurde PV, Kharkar VR, Kalsi HS, et al. Efficacy of Piroxicam and Tramadol for Relieving Pain Associated with Therapeutic Dental Extractions followed by Immediate Archwire Loading during Orthodontic Treatment: A Cross-Over Randomized Clinical Trial. Glob J Med Pharm Biomed Update. 2024;19:9. doi: 10.25259/GJMPBU_14_2024
Abstract
Objectives:
Extraction of premolars and archwire loading during orthodontic treatment is associated with postoperative pain that affects the patient’s quality of life and acceptability for the treatment. Prompt management of post-operative pain can improve patient’s compliance and confidence in the dental profession.
Material and Methods:
The present split-mouth double-blinded randomized clinical trial was conducted on 30 patients undergoing bilateral maxillary first premolar extraction followed by archwire placement for orthodontic treatment. Patients were administered either of the two drugs, tramadol or piroxicam, and their pain levels were recorded by visual analog scale at 2-hours (h), 4-h, and 6-h intervals. The same protocol was repeated for extraction of the contralateral premolar 1 week later, and the patients were provided with the other drug not received during the first extraction, followed by an assessment of the pain levels.
Results:
The pain levels were significantly higher (P < 0.01) at 2 h in the patients taking piroxicam as compared to 4-h and 6-h intervals. There was a significant rise in pain at the 4- and 6-h intervals compared to the 2-h interval following the administration of tramadol. The pain levels were significantly higher (P < 0.01) in the piroxicam group at the 2-h and 4-h intervals as compared to patients in the tramadol group. On the contrary, when considering the pain levels at the 6-h intervals, the pain levels were found to be significantly lower for patients administered with piroxicam.
Conclusion:
The use of piroxicam for the management of pain following the extraction and archwire placement during orthodontic treatment is more beneficial than the use of tramadol due to the sustenance of its effect over a prolonged duration of time.
Keywords
Analgesics
Post-operative pain
Dental extraction
Archwire placement

INTRODUCTION
In orthodontic practice, premolars are commonly extracted to gain space to correct malocclusions due to tooth size-arch length discrepancy or severe proclination. To mobilize the teeth such that they utilize the space gained by extraction of the premolars, an archwire is immediately loaded in orthodontic brackets for rapid retraction of the anterior teeth.[1] However, extractions are associated with post-operative pain which gets further aggravated when orthodontic forces are applied by the archwire. These forces generate areas of pressure on the periodontal ligament evoking a cascade of inflammation mediated by the release of pain-promoting cytokines such as histamines, bradykinins, serotonin, substance P, cytokines, and prostaglandins.[2] The intensity of pain increases within the first few hours following the archwire loading. The pain and discomfort can subsequently lead to a patient’s reluctance to confide in the dentist and accept treatment. Therefore, prompt management of postoperative pain is crucial to ensure adequate patient confidence in the dental professional and compliance with the treatment.
An array of methods is available at present for the management of postoperative pain related to premolar extraction with archwire loading in orthodontics. These include local anesthetic materials, analgesic drugs, low-level laser therapy, transcutaneous electric nerve stimulation, and others, with analgesics being the mainstay of pain management.[3] An important consideration is the duration of the analgesic effect, as most of these tend to have a short-term effect that diminishes over time, therefore warranting the use of longer-lasting modalities such as orally administered drugs. The onset of action, the plasma half-life of the administered drug, and side effects caused by the administration of the drug are important parameters that require due consideration.
Among the drugs, non-steroidal anti-inflammatory drugs (NSAIDs) constitute the first-line pharmacological treatment for post-extraction pain due to their ability to subdue inflammation while alleviating the pain. Although over-the-counter drugs such as ibuprofen and aspirin have been commonly prescribed for relieving post-extraction pain, the side effects associated with their use cannot be overlooked.[4] Furthermore, their relatively short duration of action (2–6 h) necessitates the intake of multiple doses throughout the day.
For cases with moderate-to-severe intensity of pain, opioid analgesics such as tramadol have proven effective. Tramadol acts on the opioid receptors, inhibiting the reuptake of serotonin and noradrenaline, thereby interrupting the transmission of pain. The half-life of tramadol being 5–6 hours warrants the need for a longer-lasting alternative for the management of moderate to severe post-operative pain.[5]
Piroxicam, an oxicam-type NSAID, inhibits prostaglandin-mediated pain and inflammation, with the plasma half-life estimated to be more than 45 h.[6] Therefore, the analgesic effect of a single dose is sustained for about two post-surgical days. The analgesic effect of piroxicam has been demonstrated to be superior to ibuprofen in patients undergoing fixed orthodontic treatment with separator placement.[7] Furthermore, the drug has fewer gastrointestinal adverse effects as compared to other NSAIDs. To date, none of the studies have compared the efficacy of piroxicam and tramadol as analgesics in the context of extractions and archwire placement during orthodontic treatment. Whether the potency of piroxicam as an analgesic in this regard is on par with that of tramadol requires exploration.
The present study, thus, aims to compare the efficacy of piroxicam and tramadol in reducing pain following extraction and archwire placement during orthodontic treatment.
MATERIAL AND METHODS
The present randomized clinical trial adopted a split-mouth design that was conducted for the duration of three months from October to December 2023. The study was conducted following the principles of New Drugs and Clinical Trials rules (2019) and the Declaration of Helsinki. The study protocol was approved by the Institutional Ethical Review Board (Protocol Ref No.: BEC392082023).
Patient recruitment and allocation
Patients within the age group of 18–35 years indicated for bilateral premolar extraction due to bimaxillary protrusion and crowding were considered eligible for inclusion in the study. Patients with systemic diseases, bleeding disorders, epilepsy, and mental disorders were excluded from the study. Patients with a history of NSAIDs, antibiotics, antihistaminics, calcium supplements, or other drugs that could affect bone remodeling or pain perception within the past week of recruitment were excluded from the study. An informed consent was obtained from those included in the study.
The patients were then randomly assigned into either of the two groups (Group I: Piroxicam and Group II: Tramadol) by computer-generated randomized codes with an allocation ratio of 1:1. The randomization and allocation procedures were performed by a laboratory assistant, while the patient and the clinician were both blinded regarding the drug provided to the patient.
Surgical procedures
All the extractions were performed under 2% lignocaine hydrochloride with adrenaline (1:80,000). Local anesthesia along with adrenaline is administered by local infiltration method to the patient. It was ensured that the extraction procedure was carried out under aseptic conditions and as atraumatically as possible. Patients who experienced traumatic extraction procedures or excessive soft-tissue lacerations were excluded from the study. A pressure pack containing cotton dampened with zinc oxide eugenol was then provided to the patients following the extraction procedure. The pressure pack was removed 1 hour following the extraction procedure, and the extraction site was cleaned and inspected for clot formation without causing any injury to the healing socket. A 0.014 Niti archwire was loaded on the maxillary dentition.
Post-operative instructions
For the following 24 hours, the patients were advised to avoid eating hard, hot, and spicy foodstuffs. They were also instructed to avoid drinking fluids, using straws, or performing any other sucking actions that could dislodge the clot from the extraction socket. Patients were also advised to cut fruits and other foods into small pieces instead of tearing them as a whole with incisors to avoid accidental breakages of brackets and prevent laceration from archwire. Relief wax was provided to the patientstoapply in case of constant friction of the terminal end of the archwire with the cheek mucosa.
Outcome assessment and second visit
The patient was asked to consider the pain level at this point as neutral (5) on a visual analog scale (VAS). Depending on the group assigned, the laboratory assistant provided them with the corresponding drug crushed into powder in a pre-formed opaque white packet. The pain levels were recorded regarding the baseline level using VAS at intervals of 2 h, 4 h, and 6 h following extraction procedures.
After 7 days, the archwire was removed and the maxillary first premolar of the contralateral side was extracted using the same protocol. The archwire was again loaded after an hour [Figure 1], and the patients were now administered the alternate drug, which they did not receive during the first extraction. The pain levels were again recorded at the 2-h, 4-h, and 6-h intervals. The patients were recalled for follow-up after 1 week. No complications were reported by any of the patients during the study.
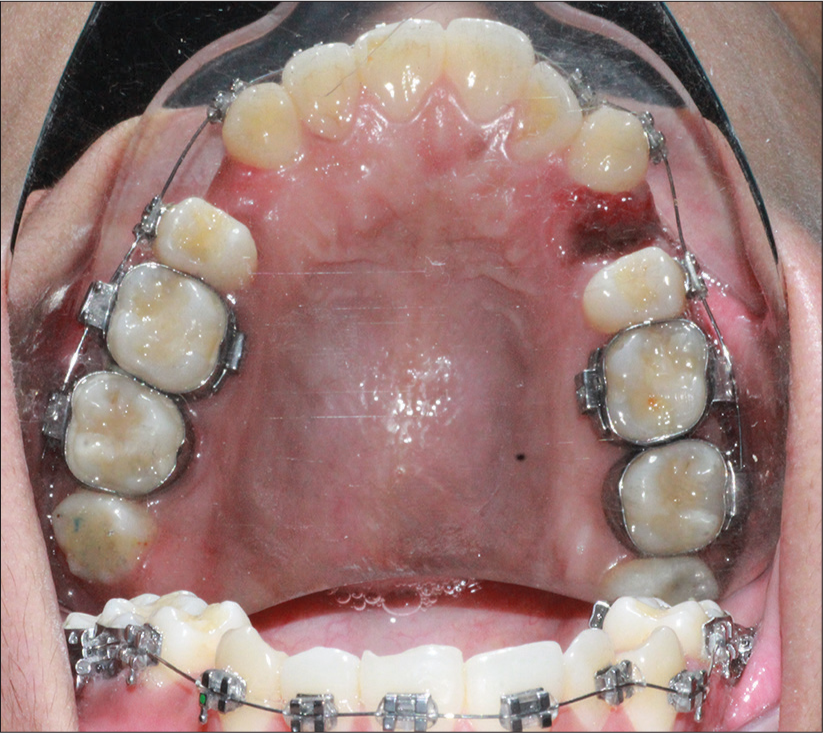
- Archwire loaded in brackets post-extraction of the maxillary first premolar.
Statistical analysis
Statistical analysis for the recorded data was performed using the Statistical Package for the Social Sciences v 26.0, IBM. Descriptive statistics were calculated in the form of frequencies and percentages for categorical data and mean and standard deviation for numerical data. The normality of numerical data was checked using the Shapiro–Wilk test which revealed that the data did not follow a normal curve, and hence, non-parametric tests were used for comparisons. Intra-group comparison of pain levels for each drug at different intervals was performed by the Friedman test, while pair-wise comparison between each interval was performed by the Wilcoxon Signed-Ranks test. Inter-group comparison of pain levels between the two groups at each interval was done by the Mann–Whitney U-test. Sub-group analysis of the pain levels at different intervals based on the patient’s gender was performed by t-test. For all the statistical tests, P < 0.05 was considered to be statistically significant, keeping α error at 5% and β error at 20%, thus setting the power for the study as 80%.
RESULTS
A total of n = 36 patients were recruited in the present study, from which n = 6 patients were excluded along the study process [Figure 2]. The final sample of 30 patients comprised 18 females and 12 males. The age of the patients ranged from 18 to 28 years, with a mean of 22 ± 3.24 years.
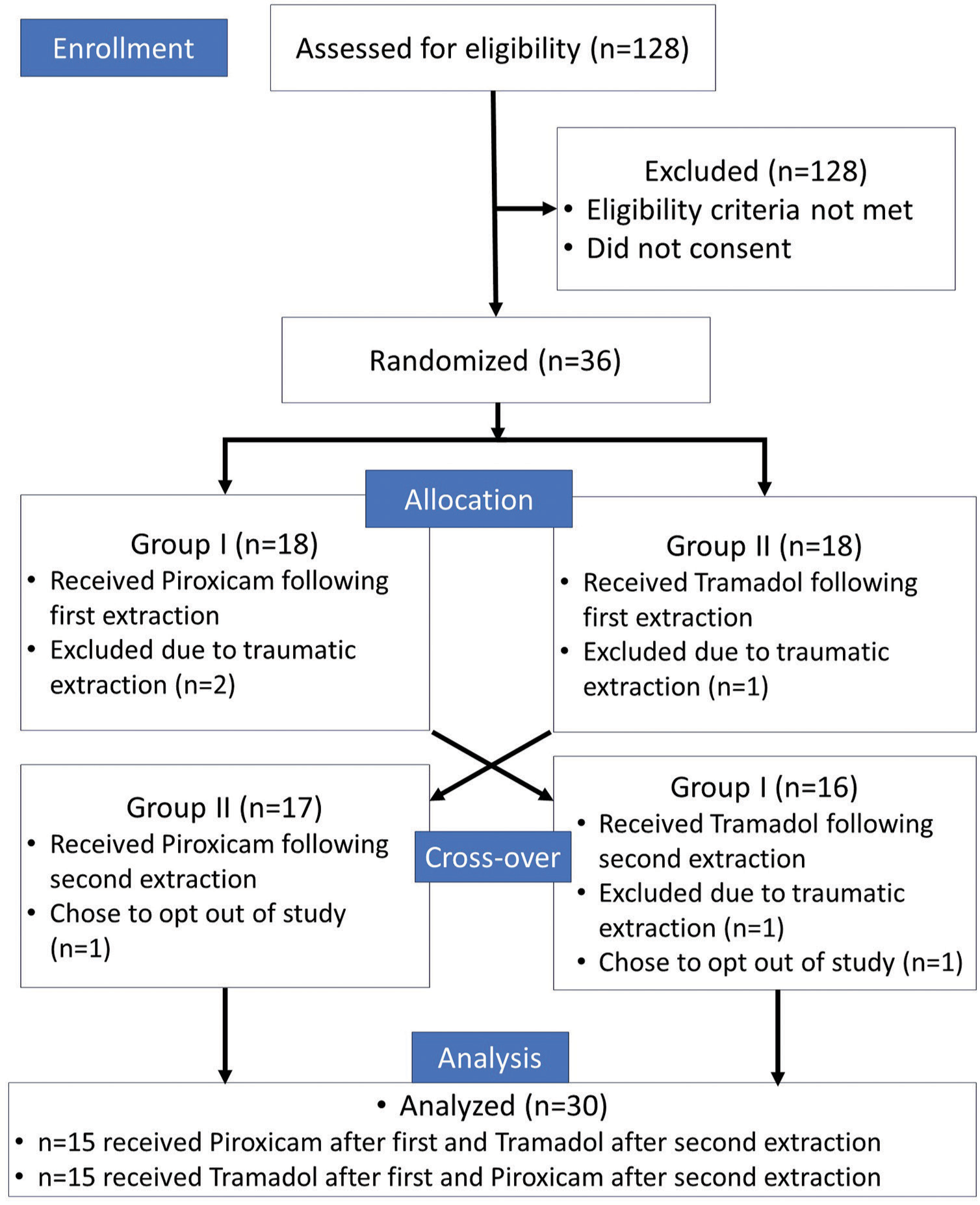
- Flow diagram indicating the process of recruitment and allocation of the patients to the point of final analysis.
On application of the Friedman test [Table 1], it was noted that the pain levels were significantly higher (P < 0.01) at 2 h in the patients taking piroxicam as compared to 4-h and 6-h intervals. This indicated that the pain levels decreased significantly as time passed after taking the drug. On the other hand, it was found that the pain levels in the tramadol group were significantly higher (P < 0.01) at the 6-h interval as compared to the 2-h and 4-h intervals.
| Drugs | Time intervals | Mean | Std. deviation | Minimum | Maximum | Median | Mean rank | Chi-square value | P-value of Friedman test |
|---|---|---|---|---|---|---|---|---|---|
| Piroxicam | 2 h | 3.17 | 0.747 | 1 | 5 | 3.00 | 2.48 | 29.431 | 0.000** |
| 2.70 | 0.988 | 1 | 4 | 3.00 | 2.25 | ||||
| 1.73 | 0.521 | 1 | 3 | 2.00 | 1.27 | ||||
| Tramadol | 2 h | 1.63 | 0.490 | 1 | 2 | 2.00 | 1.00 | 48.500 | 0.000** |
| 3.50 | 0.731 | 3 | 5 | 3.00 | 2.43 | ||||
| 3.80 | 1.064 | 2 | 6 | 4.00 | 2.57 |
Pair-wise comparisons [Table 2] revealed that the reduction achieved by piroxicam was significant (P < 0.05) between each 2-hourly interval. The reduction in the pain levels at the 6-h interval was highly significant as compared to those recorded at 2 h post-extraction (P < 0.01). For the tramadol group, there was a significant rise in pain at the 4-hour interval as compared to the 2-hour interval. Although the pain levels further increased at the 6-hour interval, the difference failed to reach statistical significance (P > 0.05).
| Time pairs | Z value | P-value of wilcoxon signed ranks test |
|---|---|---|
| Piroxicam | ||
| 4 h–2 h | −1.972 | 0.049* |
| 6 h–2 h | −4.460 | 0.000** |
| 6 h–4 h | −3.795 | 0.000** |
| Tramadol | ||
| 4 h–2 h | −4.860 | 0.000** |
| 6 h–2 h | −4.841 | 0.000** |
| 6 h–4 h | −1.346 | 0.178# |
Subset analysis of patients based on their gender for pain levels at different post-extraction intervals following the administration of the two drugs revealed statistically non-significant differences (P > 0.05) except in the piroxicam group wherein females showed significantly lower mean levels of pain (P < 0.05) as compared to males at the 6-h interval [Table 3].
| Group | Post-extraction interval | Gender | n | Mean | Std. deviation | Std. error mean | t-value | P-value of t-test |
|---|---|---|---|---|---|---|---|---|
| Piroxicam | 2 h | M | 12 | 3.33 | 0.651 | 0.188 | 0.998 | 0.900# |
| F | 18 | 3.06 | 0.802 | 0.189 | ||||
| 4 h | M | 12 | 2.58 | 1.084 | 0.313 | −0.521 | 0.481# | |
| F | 18 | 2.78 | 0.943 | 0.222 | ||||
| 6 h | M | 12 | 1.67 | 0.651 | 0.188 | −0.566 | 0.040* | |
| F | 18 | 1.78 | 0.428 | 0.101 | ||||
| Tramadol | 2 h | M | 12 | 1.58 | 0.515 | 0.149 | −0.450 | 0.421# |
| F | 18 | 1.67 | 0.485 | 0.114 | ||||
| 4 h | M | 12 | 3.33 | 0.651 | 0.188 | −1.020 | 0.194# | |
| F | 18 | 3.61 | 0.778 | 0.183 | ||||
| 6 h | M | 12 | 3.33 | 1.155 | 0.333 | −2.071 | 0.414# | |
| F | 18 | 4.11 | 0.900 | 0.212 |
The Mann–Whitney U-test [Table 4] revealed that the pain levels were significantly higher (P < 0.01) in the piroxicam group at the 2-hour and 4-hour intervals as compared to the patients in the tramadol group. On the contrary, when considering the pain levels at the 6-hour intervals, the pain levels were found to be significantly lower for patients in the piroxicam group as compared to those in the tramadol group.
| Time intervals | Group | n | Mean | Std. deviation | Mean rank | Sum of ranks | Mann–Whitney U-value | Z-value | P-value of Mann– Whitney U-test |
|---|---|---|---|---|---|---|---|---|---|
| 2 h | Piroxicam | 30 | 3.17 | 0.747 | 44.05 | 1321.50 | 43.500 | −6.279 | 0.000** |
| Tramadol | 30 | 1.63 | 0.490 | 16.95 | 508.50 | ||||
| 4 h | Piroxicam | 30 | 2.70 | 0.988 | 24.43 | 733.00 | 268.000 | −2.967 | 0.003** |
| Tramadol | 30 | 3.50 | 0.731 | 36.57 | 1097.00 | ||||
| 6 h | Piroxicam | 30 | 1.73 | 0.521 | 16.75 | 502.50 | 37.500 | −6.327 | 0.000** |
| Tramadol | 30 | 3.80 | 1.064 | 44.25 | 1327.50 |
DISCUSSION
The objective of the present study was to evaluate the efficacy of piroxicam over tramadol in relieving pain following the extraction of premolars and immediate arch-wire loading for harnessing the advantage of rapid retraction during orthodontic treatment. The patients recruited in the present study were mainly young adults in the age range of 18–28 years. This age group constitutes the majority of the patients seeking orthodontic treatment to resolve esthetic and functional concerns related to malocclusions.[8,9] In addition, the response to orthodontic treatment and subsequent healing can be optimally observed in patients belonging to this age group. Younger patients in developing stages may exhibit exaggerated and varied responses influenced by hormonal levels. On the other hand, the response may be diminished in older individuals due to lower metabolic rates and cell senescence.[10,11]
The results of the present study indicated that both drugs achieved satisfactory post-operative analgesia for a duration of 2 h. The pain levels recorded in the patients administered with tramadol were significantly lower at the 2-h post-extraction interval as compared to those administered with piroxicam. This indicates that tramadol can achieve a potent analgesic effect more rapidly than piroxicam. Our findings contradict those from an earlier study that observed a superior analgesic effect of piroxicam over tramadol even after a 2-h duration.[7] However, the pain levels following the intake of tramadol exhibited a rise in the following two intervals (4-h and 6-h) at which the pain was recorded. This points toward the fact that although the drug was able to achieve a relatively more rapid onset of action, the effect lasted for a shorter duration leading to a higher consumption of rescue medication doses.
On the contrary, a decline in the intensity of pain was observed following the administration of oral piroxicam. The significant reduction in pain levels every 2 h following the administration of piroxicam indicates that the drug has a longer-lasting analgesic effect than its comparator. This observation was consistent with the report from an earlier study that found 20 mg of piroxicam to significantly reduce pain intensity and increase the time for the first analgesic as compared to 100 mg tramadol.[12] Piroxicam, being an oxicam type of drug, has a plasma half-life of more than 45 h which accounts for the relatively longer duration of its clinical effects.[6] Further, support for this fact was provided by Isiordia-Espinoza et al., who reported a higher time to the first analgesic in patients taking oral meloxicam as compared to those administered with tramadol following mandibular third molar extraction.[13] However, a contradictory finding was reported by Desai et al. wherein the pain experienced by the patients in their study increased gradually from 2 to 48 h following the administration of piroxicam.[14]
In the present study, the intergroup comparison showed that pain levels in the patients administered with tramadol were lower than those administered with piroxicam at the 2-h and 4-h intervals. On the other hand, piroxicam exhibited a superior analgesic effect at the 6-h interval as compared to tramadol. This analgesic effect was even more accentuated for females as revealed by gender-based comparisons. A possible reason for the increased efficacy of the drug could be due to the lower body-mass index in females leading to increased apparent volume of distribution of the drug.[15]
The Mann–Whitney U-test [Table 4] revealed that the pain levels were significantly higher (P < 0.01) in the piroxicam group at the 2-h and 4-h intervals as compared to patients in the tramadol group. However, when considering the pain levels at the 6-h intervals, the pain levels were found to be significantly lower for patients in the piroxicam group as compared to those in the tramadol group.
It has been reported that piroxicam administered by the sublingual route is more efficacious in reducing pain 6 h post-extraction as compared to the oral route.[16] Future studies can take the route of administration of piroxicam into account. Nevertheless, the sustenance of the analgesic effect of piroxicam over a prolonged duration can help eliminate the need for a second prescription to the patient, which is at times advised following the first archwire loading until the patient is acclimatized to the brunt of forces subjected by orthodontic wires. The effective and sustained pain control achieved by piroxicam in this regard would enable orthodontists to harness the benefits of empty sockets for rapid retraction, thereby enhancing treatment outcomes.
An inherent limitation of NSAIDs is that they exert an inhibitory action on the orthodontic tooth movement by their property to reduce inflammation and subsequently, bone resorption.[17,18] This aspect of NSAIDs warrants further investigation and comparison with other classes of drugs as analgesics during orthodontic treatment. An opposite of this effect is the regional acceleratory phenomenon (RAP) that hastens the bone remodeling process mediated strain-induced release of cytokines.[19,20] The loading of the archwire immediately following extraction produces an effect similar to the RAP.
None of the patients reported any adverse effects related to either of the two drugs in the present study. However, this was because the observation period was only 6 h while adverse effects would generally be noted after taking multiple doses of a drug. A short observation period and small sample size, thus, constitute limitations of the present study. Further studies with longer observation periods are warranted to ascertain the safety profile of both drugs.
CONCLUSION
Piroxicam can be used effectively to reduce post-operative pain following extraction and archwire placement during orthodontic treatment. The longer duration of its effect eliminates the need for multiple doses of drugs in the post-operative days and improves patient compliance and acceptability for orthodontic treatment. The orthodontic treatment outcome would be enhanced by enabling clinicians to harness the benefits of rapid retraction through effective pain control. It would also reduce the adverse effects associated with other types of pharmacological treatment although its effect on the orthodontic tooth movement warrants consideration through future studies. Hence, the use of piroxicam for the management of pain following the extraction and archwire placement during orthodontic treatment is more beneficial than the use of tramadol due to the sustenance of its effect over a prolonged duration of time.
Ethical approval
The research/study was approved by the Institutional Review Board at Bharati Vidyapeeth (Deemed to be) University Dental College and Hospital, Navi Mumbai, number BEC392082023, dated August 09, 2023.
Declaration of patient consent
The Authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Accelerated Orthodontic Treatment-What's the Evidence? Aus Dent J. 2017;62:63-70.
- [CrossRef] [PubMed] [Google Scholar]
- The Role of Cytokines in Orthodontic Tooth Movement In: Current Approaches in Orthodontics. Norderstedt: BoD-Books on Demand; 2018. p. :361-9.
- [CrossRef] [PubMed] [Google Scholar]
- Comparative Study of Effects of LASER, TENS, and Anesthetic Gel for Controlling Pain after Placement of Elastomeric Separators: A Clinical Trial. Int J Clin Pediatr Dent. 2020;13(Suppl 1):S82-6.
- [CrossRef] [PubMed] [Google Scholar]
- The Efficacy of Analgesics in Controlling Orthodontic pain: A Systematic Review and Meta-Analysis. BMC Oral Health. 2020;20:259.
- [CrossRef] [PubMed] [Google Scholar]
- Trends in Tramadol: Pharmacology, Metabolism, and Misuse. Anesth Analg. 2017;124:44-51.
- [CrossRef] [PubMed] [Google Scholar]
- Goodman and Gilman's The Pharmacological Basis of Therapeutics. (11th ed). New York: McGraw Hill; 2006.
- [CrossRef] [Google Scholar]
- Effectiveness of Piroxicam and Ibuprofen Premedication on Orthodontic Patients' Pain Experiences: A Randomized Control Trial. Angle Orthod. 2011;81:1097-102.
- [CrossRef] [PubMed] [Google Scholar]
- Orthodontic Treatment Need in 13-30 Years Patients by Using the Index of Orthodontic Treatment Need. Pak Oral Dent J 2010:30.
- [Google Scholar]
- Factors Affecting the Duration of Orthodontic Treatment: A Systematic Review. Eur J Orthod. 2008;30:386-95.
- [CrossRef] [PubMed] [Google Scholar]
- Age Effect on Orthodontic Tooth Movement Rate and the Composition of Gingival Crevicular Fluid. J Orofac Orthop. 2020;81:113-25.
- [CrossRef] [PubMed] [Google Scholar]
- Age-Dependent Biologic Response to Orthodontic Forces. Am J Orthod Dentofacial Orthop. 2018;153:632-44.
- [CrossRef] [PubMed] [Google Scholar]
- Pre-Emptive Analgesia Efficacy of Piroxicam Versus Tramadol in Oral Surgery. J Dent Anesth Pain Med. 2022;22:443-50.
- [CrossRef] [PubMed] [Google Scholar]
- Pre-Emptive Analgesic Effectiveness of Meloxicam Versus Tramadol after Mandibular Third Molar Surgery: A Pilot Study. J Oral Maxillofac Surg. 2012;70:31-6.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of Analgesic Effect of Piroxicam and Transcutaneous Electrical Nerve Stimulation Therapy on Pain associated with Orthodontic Separator Placement: A Single Blind Randomized Controlled Trial. World J Dent. 2018;9:284-290.
- [CrossRef] [Google Scholar]
- Effects of Age and Sex on Piroxicam Disposition. Clin Pharmacol Therap. 1985;37:13-8.
- [CrossRef] [PubMed] [Google Scholar]
- Sublingual Piroxicam-A Painless Way in the Management of Lower Third Molar Extraction. J Pharm Negative Results. 2022;13:278-83.
- [CrossRef] [Google Scholar]
- NSAIDS (Non-Steroidal Anti-Inflammatory Drugs)-Their Effects and Side Effects in Orthodontic Therapy-A Review. Dent J Adv Stud. 2017;5:8-13.
- [CrossRef] [Google Scholar]
- Drugs Influencing Orthodontic Tooth Movement: An Overall Review. J Pharm Bioallied Sci. 2012;4(Suppl 2):S299-303.
- [CrossRef] [PubMed] [Google Scholar]




