Sir,
A 16-year-old female presented to us with history of breathlessness for 2 weeks and chest discomfort for 4 days. Breathlessness was gradually progressive from NYHA Grade II to Grade IV at presentation. There was no history of angina pain, cough, paroxysmal nocturnal dyspnea or hemoptysis.
Examination revealed pulse - 100/min, blood pressure - 70/50 mm Hg, JVP raised with prominent ‘x’ descent and non-pitting edema of feet. There was presence of facial puffiness also with coarsening of facial features, dry brittle scalp hair, thick lips, dry and scaly skin and hoarseness of voice (features characteristic of hypothyroidism - Figure 1).
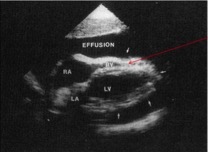
CVS examination showed distant heart sounds, tachycardia and no murmur. Respiratory and Abdomen system examinations were within normal limits. Chest X-ray showed cardiomegaly with positive hilum onlay sign (Figure 2). ECG showed low voltage complexes with tachycardia. A 2D- echo revealed large pericardial effusion with right ventricular diastolic collapse, suggestive of tamponade with ejection fraction - 25 % (Figure 3).
 |
 |
 |
|---|---|---|
| Figure 1: Hypothyroid facies | Figure 2: CXR showing Cardiomegaly | Figure 3: 2D Echo parasternal long axis (PLAX) view showing large pericardial effusion |
In view of tamponade, pericardiocentesis was performed and a pigtail catheter was inserted. Around 1000 ml of pericardial fluid was drained and the patient improved significantly. The drain was kept in situ for 4 more days and later removed. Examination of pericardial fluid confirmed transudate nature of fluid, with triglyceride levels 140mg/dl. Pericardial fluid analysis showed pH 7.2, LDH 713, Sugar 83, Protein 5.8, TLC 112/cumm, RBC 2-3, WBC 4-5, Polymorphs 70% and Lymphocyte 30%. Thyroid profile showed T3 – 24ng/dl (60-200), T4 - 2.10ug/dl (4.5-12) and TSH - >150.00uU/ml (0.30-5.5).
Pericardial effusion in hypothyroidism is mainly due to increased capillary permeability. The fluid usually contains increased cholesterol crystals because of abnormal lipid metabolism. The quantity of the fluid correlates with the severity of hypothyroidism.1
Cardiac tamponade is a medical emergency. Bedside echocardiography is one of the gold standard investigations to diagnose pericardial effusion with cardiac tamponade. Hypothyroidism presenting with massive pericardial effusion with cardiac tamponade is an uncommon presentation as in the present case report. How rapidly pericardial fluid gets accumulated is more important as far as cardiac hemodynamics is concerned rather than the volume of effusion. Mild pericardial effusion usually responds to thyroxine supplementation therapy, but tamponade requires immediate pericardiocentesis.1,2
REFERENCES
- Retnam VJ, Chichgar JA, Patkar LA, Chikhalikar AA, Golwalla AF. Myxedema and pericardial effusion with cardiac tamponade (a case report). J Postgrad Med. 1983;29:188-90B.
- Chou SL, Chern CH, How CK, Wang LM, et al. A rare case of massive pericardial effusion secondary to hypothyroidism. J Emerg Med. 2005;28:293-6.
Dr. Sourya Acharya
Professor, Department of Medicine
JawaharLal Nehru Medical College
D.M.I.M.S (Sawangi), Wardha
Maharashtra, India
Email: souryaacharya@yahoo.co.in