INTRODUCTION
Liver is often the first and only site for metastatic spread in colorectal malignancies. The mean survival in untreated patients is less than 1 year. Patient survival beyond 3 years is uncommon and virtually no patient is alive at 5 years [1]. Until recently patients diagnosed to have hepatic colorectal metastasis were viewed with little hope. However with the increasing safety of hepatectomy, surgical resection of such liver metastases has become standard therapy.
Although such resections for colorectal liver metastasis are commonly performed in specialized centres in the West, such extensive resection has never been reported from centres in India.
CASE DETAILS
A 27 year male presented with a history of bleeding Per Rectum, alteration of bowel habit and weight loss for 9 months. On examination he was found to have firm hepatomegaly. Colonoscopy revealed a circumferential ulcerated growth in the sigmoid colon 18 cm from the anal verge with craniocaudal extent being 5 cm. Biopsy revealed adenocarcinoma. Contrast Enhanced Computed Tomography scan of upper abdomen showed multiple calcified, partly enhancing lesions in the liver suggestive of secondaries.
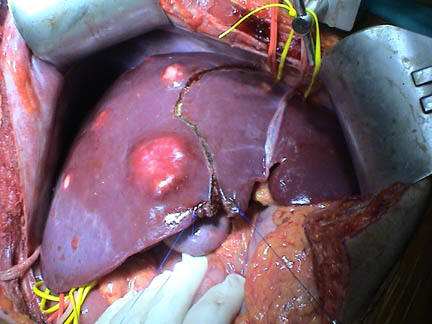
At surgery he was found to have a 5 x 6 cm size mass in the sigmoid colon. There were enlarged lymph nodes along the Inferior mesenteric vein and at the origin of inferior mesenteric artery. There were no peritoneal or pelvic deposits. Intraoperative Ultrasound revealed multiple metastatic nodules in the right lobe of the liver (Figure 1). Segment VI had only two surface nodules. There were two nodules at the junction of the middle and right hepatic veins and one on the surface of segment IV B. The superior part of the caudate lobe was involved with a 6 x 5 cm sized necrotic space occupying lesion. The left lateral segment of the liver was free.
 |
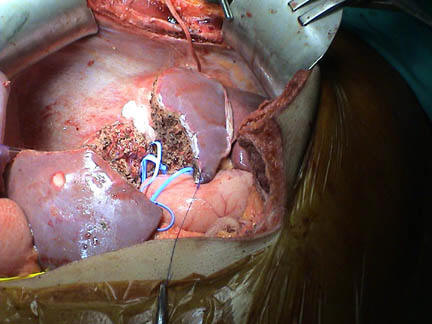
After establishing the resectability of the colonic lesion, an extended right hepatectomy sparing segment VI was performed (segments V, VII, VIII, IV B and cranial half of caudate lobe) (Figure 2). Surface nodules from segments VI and IV B were resected with 1 cm margin. The total residual liver volume was estimated to be 300 cc (Figure 3). Intra-operative cholangiogram confirmed the patency of Left hepatic duct and segment VI duct. Then anterior resection with a stapled colorectal anastomosis and a covering loop ileostomy was done along with en bloc para-aortic lymphadenectomy.
 |
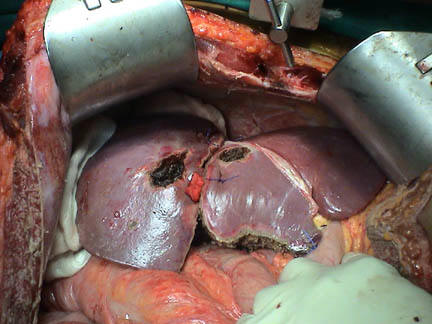 |
Figure 2: Showing extent of liver resection |
Figure 3: Showing liver after complete resection |
Histopathological examination revealed moderately differentiated adenocarcinoma colon (pT3N2M1), with involvement of muscularis propria and pararectal tissues by the tumor; the margins of resection were free. 9 out of 10 lymph nodes removed showed metastatic deposits of tumor. None of the 6 para aortic lymph nodes showed evidence of tumor metastasis. Multiple metastastic nodules were present in all the specimens of resected liver but margins of resection were free.
Post operatively the patient required intensive care with ventilatory support for 4 days. Ileostomy closure was done on day 18 and the patient was discharged in a good condition after 24 days. He has received adjuvant combination chemotherapy with oxaliplatin + 5 FU + leucovorin in 21 day cycles (one cycle every 21 days) for a total period of 6 months. He has been in regular follow up for last 48 months. Now the CEA level is 5.4 and there is no evidence of regional or local relapse on a Positron Emission Tomography scan.
DISCUSSION
The requirements recommended for synchronous of colorectal liver metastasis are [2]:
- Metastatic lesions that can be removed by a limited resection
- Medical status that would permit both procedures
- A surgeon who is comfortable in proceeding with the synchronous resection
The absolute contraindications to resection of disease metastatic to the liver are inability to resect the tumor completely, the presence of metastatic disease involving hepatic or celiac nodes, or unresectable extrahepatic disease. The relative contraindications to resection are finding multiple nodules (more than 4) or a tumor size that would require an extended resection [3]. In a recent series of 1001 liver resections at Memorial Sloan Kettering Cancer Centre, a multivariate analysis identified five adverse factors that influences outcome. These included size greater than 5 cm, disease free interval less that 1 year, more than one primary or secondary tumor, lymph node positive primary tumor and a CEA > 200 ng/ml [4].
There is general agreement that a minimum margin of 1 cm should be achieved [5]. An R0 resection is an absolute prerequisite of 5-year survival. Multiplicity of lesions [6] and the intrahepatic tumor distribution [7] both seem to be of minor importance after an R0 resection.
Although such resections for colorectal liver metastasis are commonly performed in specialized centres in the West, such extensive resection has never been reported from centres in India. Our group has performed this surgery with a curative intent and achieved a good result. The patient is still alive and disease free at 48 months post operatively. With prevailing low morbidity and mortality rates of modern day surgery we recommend synchronous resection of colorectal liver metastasis in a select group of patients in dedicated centres with specialized expertise in hepatobiliary surgery.
REFERENCES
- Wagner JS, Adson MA, Ilstrup DM. The natural history of hepatic meatastasis from colorectal cancer. Ann Surg. 1984;199:502-8.
- Jamison RL, Donohue JH, Nagorney DM, et al. Hepatic resection for metastatic colorectal cancer results in cure for some patients. Arch Surg. 1997;132:505-11.
- Wanebo HJ, Chu QD, Vezeredis MP, et al. Patient selection for hepatic resection of colorectal metastases. Arch Surg. 1996;131:322-9.
- Fong Y, Fortner J, Sun RL, et al. Clinical score for predicting recurrence after hepatic resection for metastatic colorectal cancer: Analysis of 1001 consecutive cases. Ann Surg. 1999;230:309-21.
- Registry of Hepatic Metastasis. Resection of the liver for colorectal carcinoma netastasis. A multi - institutional study of indications for resection. Surgery. 1998;103:278-88.
- Scheele J, Stangl R, Altendorf-Hofmann A. Hepatic metastasis from colorectal carcinoma: impact of surgical resection on the natural history. British Journal of Surgery. 1990;77:1241-6.
- Ekberg H, Tranberg KG, Andersson R et al. Determinants of survival in liver resection for colorectal secondaries. British Journal of Surgery. 1986;73:727-31.