INTRODUCTION
Smoking is socially accepted in various communities and cigarette consumption has drastically increased around the world [1]. Recent study carried out by a local research body, indicated an increase in the rate of teenage smokers [2]. Harmful effects of smoking appear at an early age, seriously affecting the brain, gastrointestinal systems, immune functioning and respiratory systems [3]. Dependency of smoking also develops very rapidly, which might not be expected by new consumers [4]. It has been estimated that smoking will kill about 10 million people by the year 2020, if current trend of smoking persists [5].
Smoking is associated with many unwanted effects and can predispose one to a multitude of disease such as atherosclerosis [6], and dyslipidaemia [7]. Cigarette smoke is also a potent source of free radicals [8] which can also deplete scavengers of reactive oxygen species (ROS), accentuating oxidative damage [9]. The free radicals produced physiologically, have the propensity of oxidizing LDL, thereby increasing risk of atherogenicity [10]. Smokers generally demonstrate increased level of pseudo halide thiocyanate (SCN) [11], a major risk factor for cardiovascular diseases. SCN can in turn enhance the activity of myeloperoxidase by acting as a catalyst at the same and thereby leading to oxidation of LDL [12].
Coronary heart disease is a multifactorial disease, which can be caused by both genetic and environmental factors [13]. Though CVD is a major cause of mortality and morbidity worldwide, the incidence rate varies between ethnicities [14]. Genetic variations can also influence the propensity for the initiating event, the progression of a clinical disease state and the trajectory of the disease [15].
Mauritius being a multiethnic country carries a certain probability of genetic variation. Previous cross sectional studies indicated divergence and ethnic susceptibility among the Mauritians, influencing disease progression [16]. The aim of the current study was to investigate the effect of smoking on cardiovascular parameters between Asian and African ethnic groups, and a possible preponderance to CVD.
METHODOLOGY
Population sample
Study sample was taken from two ethnic groups of Mauritius: Asian and African type population depending on their country of origin. Each group included 30 smokers and 30 non-smokers. The volunteers were initially screened for any complications such as cardiovascular complications, diabetes and kidney insufficiency and any history of medication. Any volunteer with a history of hypertension or hospitalization following high blood pressure was excluded from the study. History of smoking and number of cigarettes was evaluated in each subject. Volunteers smoking more than 5 cigarettes per day were labeled as smokers. Non smokers were those who had never smoked. The population sample included volunteers aged between 25-45 years. A signed consent form was obtained from the volunteers prior to the study.
Statistical analysis
Results were interpreted by using SPSS software 10.0.
RESULTS
Cholesterol level among male smokers and non-smokers from different ethnicities
Cholesterol is a significant marker in CVD and due to lipolysis which occurs from smoking, as discussed earlier; we decided to assess the level of cholesterol in both groups. Mean cholesterol levels in African smokers and Non smokers were 4.65±0.88 and 4.40±1.18 respectively. Corresponding mean values among Asian smokers and non-smokers were 5.56±1.09 and 4.33±1.31. Smoker population had a higher mean cholesterol level in both groups. Difference in cholesterol level between smokers and non-smokers from the African type population was lower in comparison to the Asian population. Smoking was observed to have a greater influence on the circulating cholesterol level among Asian smokers in comparison to the African smokers. (Figure 1)
 |
Triglycerides level among male smokers and non-smokers from different ethnicities
Smoking is considered to affect the triglyceride level due to the secretion of catecholamines, which cause lipolysis. Genetically there may be an influence on the level of circulating triglycerides in different ethnicities. The mean circulating triglyceride level was observed to be 1.17±0.75 and 1.35±1.18 mmol/L respectively among African smokers and non-smokers. Corresponding values among Asian population were 2.13±1.70 and 1.70±1.82 respectively. TG level was observed to be lower among African smokers, in comparison to Asian smokers. Though the difference in TG was not significant, smoking was observed to influence circulating TG level among Asian smokers, which is comparatively higher with respect to the African population, predisposing Asian smokers to, predisposes Asian smokers to dyslipidaemia. (Figure 2)
 |
HDL cholesterol Level among male smokers and non-smokers from different ethnicities
HDL is a carrier, involved in the reverse transport of cholesterol from cells to the liver. It can also be said to act as scavenger for the body cholesterol and blood wall vessel. The HDL level was measured in both communities to assess the possible genetic interplay and role of smoking on HDL expression. Among the Asian smokers and non smokers, the HDL level was observed to be 0.67±0.11 and 0.92±0.19 mmol/L respectively. Corresponding values in the African study population was observed to be 1.18±0.42 and 1.93±0.37 mmol/L respectively. Results from our study indicate that the HDL-C level was higher among the African Non smokers in comparison to Asian Non smokers. Smoking altered the circulating HDL-C in both African and Asian origin smokers, with a more obvious lowering in the Asian smokers category. (Figure 3)
 |
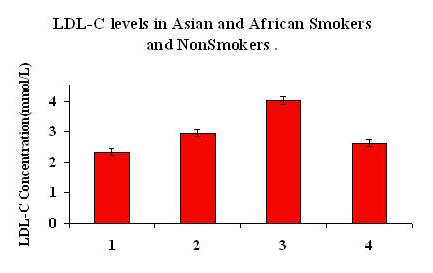
LDL cholesterol level among male smokers and non-smokers from different ethnicities
LDL is rich in cholesterol and its esters and is actively involved in the delivery of cholesterol to the extra hepatic tissues and also regulates its synthesis. We investigated the role of smoking on the LDL level and also whether there was any difference in the LDL level between two ethnic groups in Mauritius. The mean LDL level in Asian smokers and non-smokers were 4.02±0.93 and 2.63±0.85 respectively. Corresponding values in African smokers and non-smokers were observed to be 2.33±0.67 and 2.95±0.75 respectively. The LDL level was significantly raised among the Asian smokers as compared to the non smokers. (p=0.003). On the other hand, smoking was observed to lower the level of LDL in African study population. (Figure 4)
 |
APO- A1 level among Mauritian African and Asian male smokers and non-smokers
APO A1 is a lipophilic apoprotein, which efficiently effluxes tissue cholesterol and, which is then esterified and eliminated by the liver. We investigate the APO A1 level in both study populations with the view to have a better picture of the mechanisms influenced by smoking. The APO A1level in Asian smokers and non smokers was observed to be 145.90±9.59 and 159.10±16.08 respectively. Corresponding values in the African population was observed to be 172.50±15.51 and 170.0±18.0. The APO A1 level was significantly reduced in Asian smokers in comparison to non smokers (p=0.029). On the other hand, African smokers demonstrated a higher APO A1 level in comparison to the non smoker. (Figure 5)
 |
Myeloperoxidase level between Mauritian African and Asian smokers and non-smokers population
Myeloperoxidase is an enzyme which is actively secreted by the phagocytes and which oxidizes the protein lipid and also the antioxidant component of LDL, which can initiate the atherosclerotic cascade. In view of the above variations, which occur between various ethnic groups, it was decided to study the possible role of smoking on the myeloperoxidase level. The level of the enzyme was observed to be 0.42±0.13 and 0.32±0.08 mmol/l respectively in Asian smokers and non smokers. Among African type population, enzyme level was assessed to be 0.47±0.08 and 0.50±0.018 respectively among smokers and Non smokers. The enzyme level was observed to be higher among Asian smokers, compared to non smokers, which was opposite among African study population. The difference in myeloperoxidase level between African and Asian non smokers was however significant (p=0.043). (Figure 6)
 |
Oxidised LDL level between Mauritian African and Asian smokers and non smokers
Oxidation of LDL is favored by oxidative stress. Based on above observations, since myeloperoxidase level was altered due to smoking, OxLDL was alos quantified. The level of OxLDL was measured to be 74.57±13.73 and 46.38±11.87 respectively in Asian smokers and non smokers. In African study population, oxidized LDL level was 65.11±7.38 and 72.25±17.25 mmol/L respectively in smokers and non smokers category. Oxidation of LDL was significantly higher among the Asian population, as compared to the non smokers of same ethnicity. However, oxidation of LDL was reduced among African smokers. (Figure 7)
 |
DISCUSSION
Cigarette smoking is the second cause of death in the world [17]. It is also responsible for 1 in 10 adult deaths or more that 4.9 millions deaths each year [18]. A number of adverse effects have been reported to be associated with smoking, affecting several of our physiological systems, including the cardiovascular systems, immunological systems [19], and others. Besides, cardiovascular problems are also influenced by genetic predispositions. It has been reported that African Carribeans residing in UK have a lower risk of heart disease as compared to the majority of the population [20]. Other disparities, such as glucose intolerance, central obesity, fasting TG, have also been reported among various ethnic groups [21].
This study was undertaken to investigate variations in lipoproteins and associated cardiovascular parameters which might exist between our local population of migrant Asians and Africans. The Cholesterol, triglyceride and LDL levels were observed to increase among the Asian smokers. Results of our study are in accordance with other works [7, 22]. However, in African type population, corresponding values among smokers dropped. Smoking is known to increase lipolysis by stimulation of the adrenal system, increasing catecholamine, and hence increasing the TG, free fatty acids and VLDL [23]. Such mechanism might have led to an increase in lipolysis among Asian smokers, thereby increasing circulating TG, LDL and cholesterol level. Consequently, observed decrease in circulating TG, fatty acid and VLDL among African smoker population, implies indirectly a certain reduction in the rate of lipolysis, which might be associated to a genetic down regulation of the adrenergic nervous system, hence decreasing lipolysis and also showing a protective effect.
According to WHO recommendation, individuals with a TG level greater than 1.7 mmol/L are considered dyslipidaemic. Among our study population, smoking seemed to influence dyslipidaemia among Asian smoker, which was opposite for African smokers, where as TG level was surprisingly reduced. As inferred earlier, African population seems to benefit from a certain underlying genetic effect, protecting them against deleterious effects of smoking.
HDL-C, which is an important aspect of cholesterol transfer, is known to be down regulated among smokers [24]. In the current study, mean HDL-c level has been observed to decrease in both Asian and African smoker category, with respect to the non smokers, which was in accordance to literature. However, the extent of decrease in HDL-c level was steeper among Asians smokers, predisposing them again to dyslipidaemia (HDL <0.9mmol/L).
APO A1 is another major efflux system for the tissue and arterial cholesterol. In the current study, APO A1 was considerably lower among Asian smokers, vis a vis non smokers, whereas African smokers demonstrated an increase in APO A1 level. Reduction in the APO A1 level can be a severe threat to lipid deposition in cells and arteries, predisposing to atherosclerosis. It is obvious from the trend of our results that Asian smokers may be more prone to atherosclerosis compared to African smokers.
Smoking is an established source of free radicals physiologically [25]. Excess free radicals increases oxidative stress and thus all associated complications, such as atherogenesis, endothelium damage and lipid oxidation [26, 27]. In the current study, similar trend was observed among Asian smokers, but African smokers seem to be benefited with a decrease in OxLDL level, among the African study population. Myeloperoxidase, which is also actively involved in oxidative stress, is observed to increase among Asian smokers and correspondingly reduced among African smokers, This again explains a certain protective effect conferred in African population, probably by a certain genetic interplay. It may be possible, that genetically, there may be a down regulation of the myeloperoxidase enzyme expression, decreasing oxidation of LDL, and up regulation of APO A1, thereby protecting against deleterious effects of oxidants. By contrast, such a protective mechanism is not existent among Asians.
Biochemical parameters tend to be negatively influenced among Asian smokers, which is opposite among ethnic African populations. Observations from our study could also explain previously reported high cardiovascular mortality rates in Asians in comparison to other ethnicities [28].
CONCLUSION
Smoking, owing to its free radical potential, is a serious risk factor for several complications such as cardiovascular threats, age dependent macular degeneration and others. Ethnicity has also been advocated to be a strong contender to disease progression. In the current study, it has been observed that there is an obvious disparity between the two studied ethnic groups. Ethnicity implies a difference in genetic predisposition and thus a difference in physiology. The Asian type population was observed to be more prone to cardiovascular threats as observed by the consequent alteration in the cardiovascular parameters, as a result of smoking. The Asian type populations, both smokers and non smokers, were however prone to smoking, which can be accounted by their lifestyle. By contrast, smoking among the African type population did not negatively alter the cardiovascular parameters, but however, certain parameters, were observed to be below normal range (e.g. a lowering of the LDL level). This only implies a probable genetic adaptation and protection, which might be prevalent among the African type population but not among the Asian population, thus conferring protection to the former against the deleterious consequences of smoking. The molecular mechanism leading to such disparity needs to be studied and a larger sample size study is warranted.
REFERENCES
- WHO. Gender, Health and Tobacco. Geneva: the Organisation; 2003.
- Survey of smoking, drinking and illicit drug use among secondary school students in Mauritius. Retrieved from http://www.mrc.org/
- Aoshiba K , Nagai A. Oxidative Stress, cell death and other damage to alveolar epithelial cells induced by cigarette smoke. Tobacco Induced Diseases. 2003;3(1):219-26.
- Russell MA. The nicotine addiction trap: a 40-year sentence for four cigarettes. Br J Addict. 1990 Feb;85(2):293-300.
- WHO. Why is tobacco a public health priority? Tobacco free initiative; 2005. Retrieved from http://www.who.int/tobacco/about/en/index.html
- Kannel WB. Update on the role of cigarette smoking in coronary disease. Am Heart J. 1981 Mar;101(3):319-28.
- Sharma SB, Dwivedi S, Prabhu KM, et al. Coronary risk variables in young asymptomatic smokers. Indian J Med Res. 2005 Sep;122(3):205-10.
- Ross R. The pathogenesis of atherosclerosis: a perspective for the 1990s. Nature. 1993 Apr;362(6423):801-9.
- Finkel T, Holbrook NJ. Oxidants, oxidative stress and the biology of ageing. Nature. 2000 Nov;408(6809):239-47.
- Chisolm GM 3rd. Antioxidants and atherosclerosis: a current assessment. Clin Cardiol. 1991 Feb;14(2 Suppl 1):125-30.
- Vos T, Gareeboo H, Roussety F. Ethnic differences in ischaemic heart disease and stroke mortality in Mauritius between 1989 and 1994. Ethn Health. 1998 Feb-May;3(1-2):45-54.
- Exner M, Hermann M, Hofbauer R, et al. Thiocyanate catalyzes myeloperoxidase-initiated lipid oxidation in LDL. Free Radic Biol Med. 2004 Jul;37(2):146-55.
- Scurrah KJ, Byrnes GB, Hopper JL, et al. Sex differences in genetic and environmental determinants of pulse pressure. Genet Epidemiol. 2006 Jul;30(5):397-408.
- Chaturvedi N. Ethnic Differences in Cardiovascular disease. Heart. 2003 Jun;89(6):681-6.
- Duff GW. Evidence for genetic variation as a factor in maintaining health. Am J Clin Nutr. 2006 Feb;83(2):431S-5S.
- Zil-a-Rubab, Rahman MA. Serum thiocyanate levels in smokers, passive smokers and never smokers. J Pak Med Assoc. 2006 Jul;56(7):323-6.
- Murray S. A smouldering epidemic. CMAJ. 2006 Jan 31;174(3):309-10.
- Esson KM, Leeder SR. The millennium development goals and tobacco control: an opportunity for global partnership. Geneva: World Health Organization (WHO); 2004.
- Desplaces A, Charreire J, Izard C. Effect of the gaseous phase of cigarette smoke on lymphoblastic transformation of the small human lymphocyte (preliminary observations). Rev Eur Etud Clin Biol. 1971 Oct;16(8):822-6.
- Wild S, McKeigue P. Cross sectional analysis of mortality by country of birth in England and Wales, 1970-92. BMJ. 1997 Mar 8;314(7082):705-10.
- McKeigue PM. Impaired glucose tolerance and height. BMJ. 1991 Aug 10;303(6798):365.
- Wilson PW, Garrison RJ, Abbott RD, et al. Factors associated with lipoprotein cholesterol levels: The Framingham study. Arteriosclerosis. 1983 May-Jun;3(3):273-81.
- Andersson K, Arner P. Systemic nicotine stimulates human adipose tissue lipolysis through local cholinergic and catecholaminergic receptors. Int J Obes Relat Metab Disord. 2001 Aug;25(8):1225-32.
- Kelishadi R, Sarrafzadegan N, Nadery GA, et al. Atherosclerosis risk factors in children and adolescents with or without family history of premature coronary artery disease. Med Sci Monit. 2002;8(6):425-9.
- Ross R. Mechanisms of atherosclerosis--a review. Adv Nephrol Necker Hosp.1990;19:79-86.
- Jeremy JY, Shukla N, Muzaffar S, et al. Reactive oxygen species, vascular disease and cardiovascular surgery. Curr Vasc Pharmacol. 2004 Jul;2(3):229-36.
- Yeolekar ME, Nargund MP. Free radicals in human disease and the role of antioxidants. Indian Practit. 1994;7:377-90.
- Dowse GK, Zimmet PZ, Gareeboo H, et al. Abdominal obesity and physical inactivity as risk factors for NIDDM and impaired glucose tolerance in Indian, Creole, and Chinese Mauritians. Diabetes Care. 1991 Apr;14(4):271-82.